
If you are depressed, then you have hit the right page. Here is a detailed guide for folks who are depressed. The blog covers everything you need to understand and deal with your mental illness.
I often get letters from individuals who are depressed asking me what they should do. If you go on sites like WebMD, they will tell you that depression is a serious medical condition and that you should consult with your doctor. As such, I will assume you have already heard that piece of advice. Here, I attempt to offer folks something more.
What follows is a 15-stept blog series that I have developed to serve as a guide for folks who are feeling depressed or who think they might be and are wondering what to do about it. It is written mostly from a “self-help” perspective. You do not need to be in therapy (*although please see note at the end of this post). It is probably best suited for folks in the mild-to-moderate range of “clinical depression” and who have enough “mental energy” to read and think things through.
It does not try to sell you anything, although it does recommend several books you might consider. It also does not promise you a “quick and easy cure.” It is a guide that is divided into two broad parts. The first half of the series attempts to help you first understand what depression is, and use that to connect with understanding your situation and who you are as a person. Once we go through the steps of understanding depression and how it fits for what is going on with you, then the second half moves on to explore principles of “adaptive living.”
Related: Why We Need To Be Curious About Mental Illness
These are the guides for doing things differently in the areas:
One way to think of it is as a series of encounters that build on each other. Please proceed through them at your own pace. The first set of steps can be engaged quickly. The principles, however, require a much longer time to fully digest and implement. Part of the reason for the length is that finding one’s way out of a “depressive cave” takes time (i.e., usually weeks, often months). This is because climbing out of a depressive cave usually involves learning new ideas and skills, which need to be repeated and practiced.
The posts in the front half of the series are focused primarily on helping you identify the “neighborhood” of depression in which you are located. They involve learning about depression, about your life, and fostering understanding of your situation. The back half of the series focuses more directly on active steps you might take to move out of that neighborhood and into a more fulfilling place. The working assumption, supported by research evidence, is that it is possible for folks to find their way out of the cave of depression. It is, however, hard and takes effort and an adaptive attitude.
Although this blog series has many episodes, it does have a primary take-home message. It is as follows:
Depression is a state of behavioral shutdown that can happen for a host of reasons. The key thing to understand is that, as a state of behavioral shutdown, depression traps people into vicious cycles of avoidance and withdrawal. This means that you need to:
- Learn about the cycles of behavioral shutdown.
- Understand how they trap you, given who you are and the kinds of things that are driving your depression.
- Learn how to engage the world in a different way (i.e., doing, thinking, feeling, and relating).
Understanding what is going on and making these changes are hard to do. However, if you are patient and persevere, and are able to find a path of positive investment that nourishes your soul, then shutdown will reverse itself.
How does one find a path to positive investment? To guide the process we will be using the three “A’s”
Awareness involves increasing your understanding about what it going on, especially in terms of your feelings, thoughts, actions, and relationships. Acceptance involves being able to hold and tolerate negative feelings and distressing situations in a measured and mindful way. Active change means trying new things, even when it is hard. We will be considering each “A” in various ways in this journey.
Related: How Changing Your Beliefs Will Make You Realize How Much Life Has To Offer
As such, this journey invites you to adopt the attitude that you are attempting to:
- Increase your awareness of who you are and of what depression is, where it comes from, and what might be done
- Work toward increasing your capacity for acceptance of what is, including painful feelings and past losses
- Increase your engagement with things, even if your first instinct is to avoid and withdraw
What To Do If You Are Depressed: A 15-Step Guide
Step 1: Realize That You Are Not Alone
We can start with a general point of awareness that is important for not just people who are depressed but for everyone in society. Depression is common. It affects people across all social groups and classes. Consider that the World Health Organization identifies depression as the single most detrimental medical-health condition of all (including cancer or heart disease in terms of its “global burden”).
There are three key points for this first step. The first is that almost everyone is affected by depression, either directly or indirectly. As such, it is crucial that we are aware of this and create a community that is aware of this. Second, it is crucial that individuals dealing with depression know that they are not alone. The experience of profound loneliness is common in depression and, as we will see, it can contribute significantly to depressive states. However, the fact of the matter is that it is something many people deal with.
Third, I hope this insight might provide you with some notions about what you can do. For example, perhaps you could join a support group, either in person or online. If you Google “depression support groups” you might find something helpful there.
Related: Jin Shin Jyutsu: Ancient Japanese Technique For Stress Relief
Emphasizing the relationship aspect brings us to one of the themes for this series, which is the attitude of “loving compassion.” This means having a deep respect for the dignity for all persons—one’s self and others—and offering the general wish that folks flourish rather than suffer. As such, I would like to end this first entry with a “metta mantra” from the Buddhist Thích Nhất Hạnh:
May I be peaceful, happy, and light in body and spirit. May I be safe and free from injury. May I be free from anger, afflictions, fear, and anxiety.
May I learn to look at myself with the eyes of understanding and love. May I be able to recognize and touch the seeds of joy and happiness in myself. May I learn to identify and see the sources of anger, craving, and delusion in myself.
May I know how to nourish the seeds of joy in myself every day. May I be able to live fresh, solid, and free. May I be free from attachment and aversion, but not indifferent.
Love is not just the intention to love, but the capacity to reduce suffering, and offer peace and happiness. The practice of love increases our forbearance, our capacity to be patient and embrace difficulties and pain. Forbearance does mean that we try to suppress pain.
Related: Thich Nhat Hanh: The Art Of Letting Go and Why It Isn’t What You Think
This concludes Step 1.
Take-home” messages:
1) Depression is a state of shutdown;
(2) we need to find a path of positive investment that is nourishing;
(3) the process involves the three “As”: Awareness, Acceptance, and Active change.
Below is Step 2, which focuses on ways of relating to depression, with a focus on awareness and acceptance, rather than resistance and conflict.
Step 2: Turn And Look At The Beast Rather Than Fight It Or Run From It
Let’s face it, depression sucks. It feels miserable, it drains one’s motivation, and it orients people to want to escape and withdraw into an inner cave. Unfortunately, withdrawal into the cave has the ironic consequence of “feeding the beast.” Because of this, we need to develop a frame that orients toward the beast, at least somewhat. That is, rather than trying to hide in the cave or trying to publicly “smile” through one’s depression, the advice I offer is to look squarely at what is going on.
A metaphor from Acceptance and Commitment Therapy (ACT) might help. Imagine yourself currently in a tug of war with the “beast” of depression. On one side is you, on the other is the beast, and between the two of you is a nasty pit. You are trying to pull the beast into the pit and be rid of him. He is trying to pull you into the pit. You are trapped in an epic struggle.
Related: 6 Concrete Ways To Improve Your Emotional Health
I am asking that you let go of the rope and simply look over at the beast standing there. Of course, doing so does not kill the beast. It is still there with you. But it also means you are not immediately fighting with it, trying to force it away. Remember, you are not alone: Imagine there are lots of people in lots of tug of wars with their beasts. Now imagine everyone letting go of the rope and then sharing with each other the fact that they have been engaged in a struggle.
The main point here is that we are shifting our attitude. Our step in this episode is to stop with a frontal assault that involves directly fighting, escaping, or trying to bury the beast that is depressed. Rather, it is about looking at it.
And, yes, in part that means living with it. This may feel scary and might well seem to be the exact opposite of what your instincts have been telling you: “After all,” you may be thinking, “I just want to be happy!”

That is understandable. But what we are starting on are the lessons of awareness and acceptance. They are not easy lessons. Finally, although you may feel alone in your cave, recall that you are not. Depression is something that, directly or indirectly, affects us all. We all need to pull together and help each other reverse the cycles of shutting down.
Related: How Changing Your Beliefs Will Make You Realize How Much Life Has To Offer
The message of Steop 2 is to reframe our initial way of relating to depression. Many struggles to fight against it. This post invites you to at least consider letting go of that direct struggle for the time being and allow yourself to accept the situation and the feelings you are dealing with.
A great Buddhist insight is that suffering is the combination of pain and resistance.
I invite you to move from resistance to a mode of greater acceptance. The next few steps in our journey are designed to help you further understand the kind of beast you are dealing with.
Let’s move on to Step 3, which is more about awareness, through understanding the “nature of the beast” which is depression, which was introduced in step 1.
Step 3: Recognize That Depression Is A State Of Behavioral Shutdown
Although depression is a common health condition, there is much confusion about what the term means. The goal in this part of the blog is to help you become clearer about what depression is. First, depression is different from “normal” grief or sadness. As this blog notes, when my dog died I was sad, but I was not depressed. Many people who are depressed don’t feel sad but may feel numb or angry or anxious and agitated.
Another area of confusion that people often get hung up on is whether depression:
1. Is a normal reaction to difficulty and loss
2. Arises because someone is being weak or having other limitations of “character”
3. Is a disease of the brain (i.e., a “chemical imbalance”) that has little or nothing to do with psychology.
Although these issues are important (and we address them in various ways in this series), they are not the best place to start when trying to understand what depression is.
Rather we need to start with a description of its most basic features. Descriptively, depression is a state of behavioral shutdown. Put in a common language, it means you feel like sht and don’t feel like doing sht. Why is this the case?
When someone is in a depressed state, there is a significant shift in the flow of mental energy away from the “positive emotional investment system” and into the “negative emotional investment system.” The positive emotional system is about being energized and open to new experiences, having a lot of curiosity and desires, and seeking and approaching “the good” (e.g., things that are emotionally nourishing like high-quality relationships, exploring interesting topics, and engaging in rewarding activities).
Related: 6 Concrete Ways To Improve Your Emotional Health
In contrast, the negative emotion system is about signaling danger and loss and avoiding and withdrawing into a defensive posture. Depression is a shift that pulls the positive emotion system down and jacks the negative emotion system up. That is people who are depressed experience increases in negative feelings like sadness, discouragement, despair, anxiety, irritability, anger, shame, and guilt. In addition, they experience less energy for engagement, exploration, pleasure, happiness, and interest. Technically, this is called “anhedonia.”
Depressed individuals also often experience fatigue, a focus on past losses, a discounting of future gains, difficulty concentrating, difficulty starting new activities, and problems with sleeping and eating. The pain is sometimes so great and the feeling of being trapped too intense that the person comes to believe that the only solution for escape is suicide.

Step 3a: Be Aware of the Two “Paradoxes” of Depression
How might this understanding help you?
First, it helps you label what is going on. For purposes of awareness, we want you to be able to make meaning out of your feelings and drives (or lack thereof). With the behavioural shutdown model, you can interpret your state of mind as a shift in your drive and psychic energy from the positive to the negative emotion system.
Second, it can help you become aware of what I call the “twin paradoxes” of depressive conditions. The first is the paradox of shutdown. This paradox refers to the fact that when you are depressed, your emotional instincts are telling you to withdraw, avoid, and retreat into a cave. But if you retreat into the cave, where does that leave you? It leaves you alone, feeling like crap, with no place to go.
This means something very important: Your instincts to escape and withdraw “paradoxically” feed the beast that is depression. This idea is key to this series. It is also key to understanding the neighbourhood of depression and how you have found yourself in it and how you might learn how to move out of it.
Third, this cycle of shutdown highlights that folks need to act and react differently than their depressive instincts tell them to act and react. But, unfortunately, as we consider this fact, we encounter another paradox of depression. As you likely know, depressive moods suck available energy from you. The last thing a depressed person has is the energy to invest in some long, drawn-out process.
We can label this the paradox of effort. To turn the cycles around, you need energy and work effort—but depressive shutdowns suck all the energy out of you. Thus, it is very hard to do what is needed.

Let me summarize this entry as follows:
Depression is, first and foremost, a state of behavioural shutdown.
This means that your energy shifts from the positive to the negative, and makes you feel like doing nothing. This results in two painful paradoxes of depression. The first is the paradox of shutdown. Your depressive instincts tell you to avoid and withdraw, but that only drives you into a cave, feeding the beast more and more.
The second is the paradox of effort, that significant effort and energy are required to not be driven into a cave, but depression saps all your energy from you.
These two paradoxes help explain why so many people fall into depressive caves. The solution to these paradoxes involves working to develop the right mindset, which in part involves pacing one’s self and being patient and focusing on moving ahead slowly and purposefully toward more valued states of being.
To help with this movement, I would like to introduce a new “attitude”. In Part I, we introduced the attitude of loving compassion for self and others. The attitude I would like to introduce here is the attitude of curiosity. Curiosity is an attitude of wonder, of learning, and of openness to ideas and to feel. A curious person tries to explore. She asks questions about what, why, how. Today’s entry was about answering some basic questions about what depression is, and how to understand some of its key “paradoxes”.
Related: Why We Need To Be Curious About Mental Illness
Thus, we can think of your willingness to read and understand this post to be in part driven by some inner curiosity. Although I know it is difficult when you are depressed, perhaps you can open yourself up to being a bit more curious about yourself, your depression, and related feelings, to others and what they are feeling, and your world across time (the past, present, and future).
We end today with a quote on the concept of curiosity from Albert Einstein:
The important thing is not to stop questioning. Curiosity has its own reason for existing. One cannot help but be in awe when he contemplates the mysteries of eternity, of life, of the marvelous structure of reality. It is enough if one tries merely to comprehend a little of this mystery every day. Never lose a holy curiosity.

In the step 4, we turn our attention to things that drive folks into shutdown mode.
Step 4. Assess Your Level Of Depression
Let’s start by reflecting on the level of your depressive shutdown. We can do this by asking how much shutdown is present and for how long. We can think of this in terms of the intensity, duration, and frequency of the symptoms.
Put in the form of questions, we can ask: How strong are the symptoms? How long do they last? How often do they occur? Probably the easiest way to get a picture of your levels of depression is to take a brief test. Here is an easy test, the PHQ 9. Please take it and see how you score, as it gives you a sense of what level of depression you are dealing with.
Note that when you take it the meaning of your scores will depend on if you are a “minimizer” or “exaggerator”. This is hard to assess if you aren’t trained, just know that a “minimizer” tends to dismiss or downplay their symptoms and an “exaggerator” tends to overshoot. For now, just note that the correct interpretation depends on how you tend to respond, but it should give you a basic idea.
Related: 10 Reasons Why People Refuse to Talk to Therapists
In addition to noting your overall severity, please take a look at the symptoms you are dealing with. These are important because they can serve as clues for areas to focus on. For example, are you having problems with sleep? If so, that might be a pattern you think about addressing, as sleep habits are key to getting the rhythms of your biology flowing smoothly. Or, if you are having trouble with negative thoughts about yourself, then a cognitive approach that focuses on adaptive thinking might be more appropriate to focus on.
The second half of this series (starting with Part VII) will bring the focus more on the kinds of things you can work to change or do differently. Right now, we remain in the “awareness” stage, so just note your overall level of depressive symptoms and the more specific domains you are having problems with.
Now let’s review terms that mental health professionals use in considering this condition. This too falls under our process of “Awareness” and is consistent with the attitude of being curious.

Let’s start with the term “clinical depression.” Perhaps you have heard of it or of “clinically significant” symptoms. “Clinical” is a professional jargon term that just refers to depressive symptoms that are causing or are associated with significant distress and difficulty functioning. It is basically a judgment call that professionals make that indicates someone is experiencing problematic or substantial symptoms of depression that could be the focus of treatment.
Another key term is a “Major Depressive Episode” (MDE). Sometimes this is what is meant by clinical depression. An MDE is a term from the Diagnostic and Statistical Manual of Mental Disorders, which is what most professionals use as the official diagnostic codebook. An MDE is defined as the presence at least five of the nine symptoms that are listed on the PHQ 9. These symptoms need to be present most of the time for a period of at least two weeks. MDEs usually last several weeks into months.
If someone meets the criteria for an MDE, they often get diagnosed with a “Major Depressive Disorder”. One key piece of information to consider is your level of severity, which is usually described in terms of “mild”; “moderate”; or “severe”. Mild is where the person barely meets the criteria for an MDE.
Such folks often have a “smiling depression,” meaning that they can hide it from others and are not necessarily obviously depressed on the outside. That is, they can go to work and function in social settings, and don’t show any motor or other gross impairments. Note that the word “mild” here is not meant to suggest that it is not important or significant. It is, after all, part of the overall heading of a Major Depression.
A moderate MDD is when functional impairment starts to become obvious. Folks in this category frequently stop doing things like going to work (at least miss a day here or there), reduce time hanging with friends, or disengage from life in other ways. Concentration is hard, sleeping or eating is often disrupted, and anyone who has much contact with the person would likely notice a difference in how they are presenting.
Severe levels of MDD are profound cases of shutdown. Here the person can’t hide it at all. They move slowly, they talk slowly, their eating, sleeping, and pattern of functioning are often completely disrupted. It is hard to see someone in a severe MDD and not conclude they are “ill” in a medical/health sense. Sometimes you might hear this described as a “melancholic” depression (see here for a discussion of it and related terms).
We should also make the distinction between “recurrent” and “single” episodes. As the words sound, a single episode means this is the first and only time someone has been depressed. Recurrent (or chronic-recurrent) refers to folks who are dealing with repeated episodes or folks dealing with depression for years.
This distinction is important in part because it relates to prognosis. A single episode generally is easier to treat and more likely to result in folks bouncing back quickly. Why is this the case? Well, there is an old saying in neuropsychology that “neurons that fire together, wire together,” and it is likely that the more time one spends in a depressive state the more that state becomes accessible. In addition, the more one has been depressed, the more vulnerable one is to relapse.
Related: 3 Most Common Mental Health Disorders In Men
We should also be clear about the difference between “bipolar” and “unipolar” depression. Bipolar is the term that professionals use when an individual has experienced a “manic” or “hypomanic” episode in the past. These are episodes of heightened energy, positive or hyper-charged mood, a decreased need for sleep, irritability, excessive goal-oriented activity, increases in risky and impulsive behavior, and in full-blown episodes, disorganized thought, delusions, and hallucinations.
The presence of the bipolar disorder is crucial to know, as it requires different kinds of medications. In addition, there are good reasons to believe that bipolar disorders likely involve significant contributions from neurobiological breakdowns or malfunctions (i.e., I see bipolar conditions as more “disease-like” in its nature than unipolar). “Unipolar” are depressive conditions that do not involve a history of manic or hypomanic episodes.
Another key thing to be aware of is the notion of “persistent” or “trait-like” depressive presentations. If you recall Eeyore from Winnie the Pooh, you will be able to conjure up what it looks like when someone has persistent depressive symptoms. In the past, this was called “dysthymia” and before that, it was labeled a “depressive personality”. This tendency toward trait-like depression is related to the broader category of what professionals call “trait neuroticism.” This refers to a person’s natural tendency to experience negative emotions.
Step 4a: Assess your level of “trait neuroticism”
If one is high on the trait neuroticism then that is important to know, as it influences where one can expect to be in terms of one’s negative feelings, even when things are going reasonably well. That does not mean that you will be depressed all the time, as a depressive episode is a different state of being than just being high in trait neuroticism.
But it does mean you will be more likely to experience negative emotions and have a harder time being “calm” in stressful situations than others. And, as we will see, that is very important to understand, because we will need to help you learn to relate to your feelings in a healthy way.
As this blog notes, it is important to know if you are high in this trait. As we will see, learning to relate to your emotions is important, and doing so can be hard if you are high on trait neuroticism. [Please, note, however, your scores on this “trait” measure will likely be higher when you are depressed than not, so if you get out of your depressive episode, it might be helpful to take the assessment again.]
Finally, I need to make a comment about what mental health professionals call “co-morbid” conditions. Co-morbid means that the individual is dealing with more than one problem or illness, and they combine to make things especially complicated. If we consider that depression is a state of behavioral shutdown, then it makes sense that it often is secondary to many other problems. And, indeed, it is highly “co-morbid” with conditions like generalized or social anxiety, personality disorders, schizophrenia, substance misuse problems, and chronic illnesses or chronic pain. Of course, all of these difficulties relate to the things in a person’s life that might be driving the shutdown.
Related: Which Of the Five Psychological Factors Is Your Most Dominant? QUIZ
In sum, today in step 4 we focused on increasing your awareness of your depression. Specifically, we emphasized getting clear on how depressed you are by taking a screening measure, we identified some key mental health terms, and we introduced the concept of trait neuroticism and pointed to some resources for understanding that concept. This is all in the service of getting to know the beast that is depressed.
In step 5, we will continue the journey and start to map more clearly your personal struggle with depression—that is, we will start to map the various ways folks get depressed, which will then allow us to map who you are and put the puzzle pieces together.
Perhaps you are frustrated to hear this. Perhaps your reaction is, “I don’t need to learn any more technical stuff, I just want to stop feeling this way!” That makes sense and we should observe you’re having that thought with compassion. Yet in compassionately observing it, we should also note that the thought goes against two of our “A” principles that are guiding us on our journey. Recall those are the principles of Awareness and Acceptance. The thought echoes the wish for the third “A”, which is Active Change.
Please note that part of what we are learning on this journey is the process of being-in-the-world. The process of being-in-the-world refers to how one is in the world, rather than where one is. The old saying, “It is the journey, not the destination” makes a point about the process. The process of being that we are cultivating is a mindful attitude of awareness and acceptance.
This involves intellectual curiosity about the world, emotional curiosity about your feelings, and a way of being in a world that is aware and attuned to the present. It also involves patience and the capacity to tolerate distress (a key facet of acceptance).
Here, in step 5, we get curious about the kinds of things that might be driving your state of behavioral shutdown. Specifically, we learn about differences between: a) depressive reactions; b) depressive disorders; and c) depressive diseases.
Step 5: Recognize Depressive Reactions, Depressive Disorders, And Depressive Diseases
If depression is a state of behavioral shutdown, then it makes sense that we should ask, with an attitude of curiosity, “What might be causing my emotional-motivational system to shut down?” I distinguish between three broad kinds of causes and classify them in terms of
1) depressive reactions;
2) depressive disorders; and
3) depressive diseases.
Each of these domains can contribute to depressive feelings, and it is very important to understand what they are and why.

Depressive reactions refer to shutdowns that follow serious “psychological injuries,” such as the death of a loved one or other major losses, such as a divorce or job loss or other major life event that is experienced as a core life failure. Depressive reactions also include shutdown responses to brutally difficult or oppressive life situations, such as living with an abusive partner or dealing with chronic pain.
Our mood/emotional systems generally react to these kinds of brutal events with avoidance and withdrawal. The key questions for you here include: Can you identify a past injury that your system is reacting to in a way that the shutdown makes sense? Are you trapped or humiliated or experiencing chronic pain such that it feels that you have no path of escape? Have you experienced a loss or failure that you can’t let go? In one of my blog, with the odd sounding title: “How depressed do you want to be?”, I explain how this unusual-sounding question gets at a key feature of depressive feelings, which is that they can be understood to be a natural consequence to a brutal situation.
Related: Mental Health: The 10 Types of Sleep Disorders
Depressive disorders are the second class of causes that drive people into depressive caves. Depressive disorders involve “maladaptive” patterns of acting, reacting, relating, and coping with stress that actually makes things worse. These are vicious cycles that drive people into dead ends.
A vicious cycle involves the following:
(a) stressors or difficulties or losses in a person’s life cause them to
(b) adjust and cope in problematic ways, which lead to
(c) more trouble functioning and greater distress that then results in
(d) even more problematic coping.
This means the cycle feeds back on itself and results in things getting worse and worse. Consider, for example, the person that uses alcohol to escape from his emotional problems. Although alcohol might take the pain away in the short term, over time things often get worse and worse. Now recall the first and second “paradoxes” of depression. The paradox of shutdown results in emotional instincts to withdraw and avoid, but this drives people into the cave and “feeds the beast.”

The paradox of effort is that depression sucks energy from you that is needed to engage in the world and reverse the cycle. The basic question here is whether your depressive reactions to stress making things worse for you. Tomorrow, in Part VI, we will introduce the concept of “neurotic loops,” which is one of the most common vicious cycles that contribute to depressive disorders.
Depressive diseases are the third class of causes. This relates to biology. Before we describe depressive diseases, we need to reflect on some basic biological considerations about depression. In terms of general biological considerations, we need to be clear that depression is “biological” in the sense that a Major Depressive Episode really does represent a fundamental shift in your biology.
Related: 5 Tips to Help You Combat Depressive State of Mood in College
Changes happen in metabolism, arousal, stress reactivity, stress hormones, biorhythms, and many other domains in the body. This is one of the many reasons that asking depressed people to just “snap out it” is misguided; it is like telling a person who has not slept for 24 hours to just stop being tired.
Of course, almost everyone understands that feeling sleepy after being awake for a long time is not a disorder. Likewise, being depressed if one is being abused or trapped in vicious psychosocial cycles can also be seen as a natural consequence. Thus, just because it is “biological” does not mean that depression is a disease. And yet it is also the case that some people are tired because they have in fact have a sleeping disorder, such as sleep apnea.
Likewise, it seems plausible that some people have neuro-biological systems that are highly sensitive and become inflamed or reactive in ways that result in folks more easily tipping into depressive shutdowns. We know a number of conditions such as hypothyroidism and vascular strokes in the left hemisphere of the brain can result in folks becoming depressed.

In addition, chronic depression creates many biological sensitivities over time. I call conditions that seem driven by malfunctioning biology to be “depressive diseases.” I am especially likely to think in these terms when someone is dealing with severe or “melancholic” depressions.
Although the nature of “depression as a disease” remains controversial, many professionals and laypeople view it this way. In addition, many people report benefiting from anti-depressant medications. In addition, there are other brain-based interventions, such as electroconvulsive therapy (ECT) and transcranial magnetic stimulation, that have reasonably good evidence for chronic and treatment-resistant depression.
Related: 6 Antidepressant Medication Myths Debunked To Help Make Meaningful Choices
In my professional opinion, if you are dealing with moderate-to-severe levels of MDD, then, in addition to considering psychotherapy, you should consider consulting with a physician and testing out whether medications or other biologically based interventions might help.
How and if such medications help and if they do or do not result in side effects varies substantially from person to person. I consider it a bit like “mental alchemy.” That is, medical doctors can “sprinkle” meds on the nervous system and hope for the symptoms to reduce. Sometimes they do, sometimes they don’t. I consider biological interventions one angle that needs to be considered in the context of the larger understanding of depression as a state of behavioral shutdown.
Today we learned more about the nature of depressive shutdowns. Specifically, we started to classify different things that can result in such shutdowns. We identified three broad classes of
1) reactions;
2) disorders and
3) diseases.
Depressive reactions refer to feelings that are a natural consequence of loss, difficulty, and failure. Understanding that there are depressive reactions allows you to ask yourself the strange-sounding question: How depressed do I want to be? The point being that our emotions and moods offer crucial information for our needs and goals and if our situation is brutal it makes sense that we would feel depressed.
Depressive disorders refer to a psychological condition where the way someone is responding to stress and acting, reacting and coping with their feelings and relationships are such that things get worse and worse in the form of vicious cycles. We also highlighted that biology plays a role both in general and some folks have symptoms that are severe enough and fail to respond to changes in the environment such that I think it is reasonable to label their conditions “depressive diseases” and to consider biological interventions.
Related: 13 Characteristics Of A Mentally Healthy Person
Earlier in this series, we noted that both professionals and laypeople are confused about depression. For a host of reasons, they get stuck debating whether we should think about depression as either a normal reaction, a psychological disorder, or a biological disease. Our behavioral shutdown model helps clarify how states of shutdown can emerge from the environment, from coping styles, and be connected to biology. Tomorrow, we return to the idea of depressive disorders and will explain one of the most common maladaptive cycles, that of a neurotic loop.
Finally, if you found today’s breakdown helpful, you might check out this blog, which uses this kind of logic to list 23 different “kinds” of depression. It might help you identify the nature of the beast that is your traveling companion.
Below is Step 6.
Step 6: Understand And Identify Neurotic Loops
Neurotic loops develop when people have negative feelings about their negative feelings. Yes, you read that correctly. You have feelings about your feelings. Today we want to get clear about why this is so, and why it drives many people into depressive caves. (Note that they are called “neurotic” because although the person is trying to cope and control in an effort to make things better, the strategies often backfire and make things worse.
To begin, let me ask you a few questions about how you think about your feelings. Do you ever fear your depressed moods and fight against them (i.e., do you play tug of war with the beast, as was mentioned in Step 2)?;
Do you ask yourself questions like “Why can’t I just be happy?” or “What is wrong with me?”; Do you fear or feel uncomfortable with certain feelings, like being vulnerable or sad or angry? Do you criticize yourself for the feelings you do have? Do you try to suppress, avoid, deny or control your feelings? Are you sometimes overwhelmed by your feelings and feel flooded by them, even as you try to escape them? If you answered “yes” to these questions, then you may well be struggling with neurotic loops.
What exactly is a neurotic loop?
It is when folks get into a battle with their feelings that leaves them depleted, stressed, and feeling even more critical about themselves. Such loops usually involve three things.
The first is a “neurotic temperament.”
As was described in Part IV, this refers to the “set point” of the negative emotion system. It relates to how sensitive you feel, how strongly you react to negative events, and how long it takes you after a stressor to return to baseline.
The second primary ingredient is the stressors you face, relative to your felt sense of security.
This refers to the real-life problems in living that threaten your core needs and leave you feeling insecure and psychologically “malnourished”. Key psychological needs include the need for safety (which is violated when folks are traumatized), the need to be connected to and valued by important others, the need for achievement and competence, the need for crucial resources (i.e., money and shelter), and the need for play, growth, and exploration.
The third ingredient relates to how folks cope and react to their feelings in these stressful and psychologically difficult circumstances.
When those secondary reactions are negative and controlling in regards to the primary feeling, then folks can find themselves in a neurotic loop.
To see what I mean, let us imagine Julie as someone who deals with depression and social anxiety and who was invited to a social gathering and gets up the courage to go (see here for a blog on social anxiety). Ten minutes into the party, she has what she feels to be an awkward conversation. Moving to an isolated part of the room and trying to look casual on the outside, she internally launches in on herself: “What is wrong with you? Why are you so sensitive? This is so easy for everyone else. You can’t even come to a gathering for ten minutes without screwing things up.”
To help understand what is going on, we can divide Julie’s mental experience into three separate but related domains. One domain is her “emotional-experiential self.” This is her nonverbal “feeling mind” that automatically tracks what is going on and directly connects her to her body. I often call this the “heart.” Julie has a “sensitive” heart relative to other people, which is the sensitive way of saying she has a neurotic temperament.
The second domain of mind is her “narrator.” This is the inner talking part of her consciousness that explains what is happening and why, and how she should be. This is the part that privately criticized her for her weakness. Finally, there is Julie’s “public self.” This is the public presentation she offers to others (the part that tries to look casual, even as she is boiling inside). The relationship between these three domains of the human mind is key to understanding much about mental health.
Internal neurotic loops involve the relationship between the domains of “the heart” and “the narrator.” To understand why these domains of mind are often in conflict, we need to recognize that they operate in very different ways. The feeling mind or heart is quite automatic, fast and reactive. It feels things based on what it perceives relative to its goals in the immediate situation. If it perceives potential threats, it will send out alarms and result in general a feeling of worry or concern and will orient toward possible bad things happening.
The narrative mind is more complicated. It not only thinks about what is happening, but it also can narrate thoughts about what ought to be. This means that when the narrator is oriented toward the heart, it can decide whether the heart is feeling the “right thing” or not. This means that if the narrator decides the heart is not feeling what it should or if it decides the feelings are dangerous, then it will become critical and controlling and try to avoid or deny the feelings.
Where does the narrator get the ideas for what an individual ought to feel? Originally, these notions come from other people, either directly or indirectly. We learn rules and roles and what we should do and feel from our families and friends growing up.
For example, it is likely that you received messages about whether or not it was “okay” to be shy or angry or vulnerable. Because people generally want to be liked and accepted, they turn those judgments onto themselves. That is, the narrator internalizes (or takes over) the real or imagined judgments of others and then tries to control the heart, often by being critical or punitive.

So what does this mean for your mental health?
To understand why this inner conflict can be such a big deal, I have folks engage in what I call the “restaurant exercise.” Here is how it works. Imagine yourself at one of those big-city crowded restaurants where folks have tables very close to each other. Now imagine yourself at one table and next to you is an adult talking to a child.
The adult represents the critical narrator that is having negative reactions to the heart, which is represented by the child. Now imagine that you overhear what the adult says to the child. To see this, we can use what Julie said to herself as an example. That is, imagine an angry, critical adult harshly saying the following to a vulnerable child: What is wrong with you? Why are you so sensitive? This is so easy for everyone else. You can’t even come to a gathering for ten minutes without screwing things up.
What do you think happens to the child?
We can be sure of one thing. The child will not respond by “snapping out of it” and thanking her mother and being more secure. Instead, the child will either shrink and submit or throw a temper tantrum.
Neurotic loops stem from this kind of “inner family conflict” playing out in your head. It is a battle between the judgmental narrator and the vulnerable heart. It is a vicious cycle because it feeds back on itself. Even if the child says “Ok, I will be quiet,” the heart is still hurting and likely is hurting even more after being criticized. Not uncommonly, there is tension and a buildup and eventually, the child/heart will “lose it.”
When that happens, negative emotions flood the system and the person becomes filled with depressive despair or rage or panic in a very painful and dysregulated and maladaptive way. Of course, if this happens it only proves to the narrator that the heart/inner child needs to be controlled. This means that the cycle gets more and more entrenched.
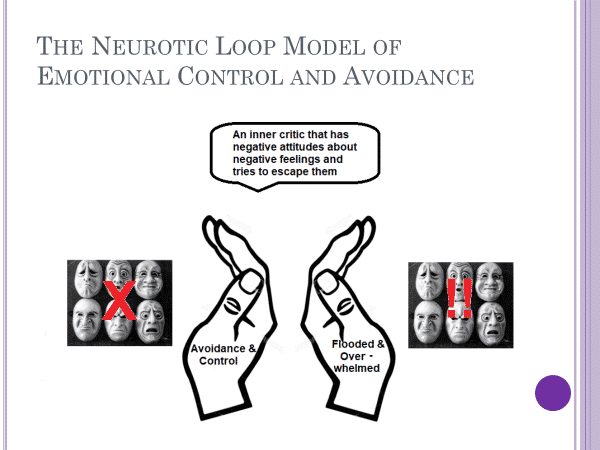
Here is a diagram I use to illustrate neurotic loops. It represents the fact that primary emotions are blocked and the narrator has a critical and controlling attitude. Sometimes, however, the emotional heart spins out of control and the person is flooded in a painful and powerful way.
Today, in Part VI, we covered the idea of neurotic loops. It involves the fact that we have three domains of mind: 1) the heart (or feeling mind); 2) the head (or inner narrator); and 3) the public self. Neurotic loops are states of inner conflict between the heart and the head (which often occur in order to manage the real or imagined judgments from others).
The task for today is to wonder whether or not you have negative reactions to negative feelings. If you answer yes, and that you often feel very differently than you wish you felt, then that is a crucial piece of information for understanding your depression. For now, just allow yourself to become aware of the fact that you have feelings and then secondary thoughts and feelings about those primary feelings.
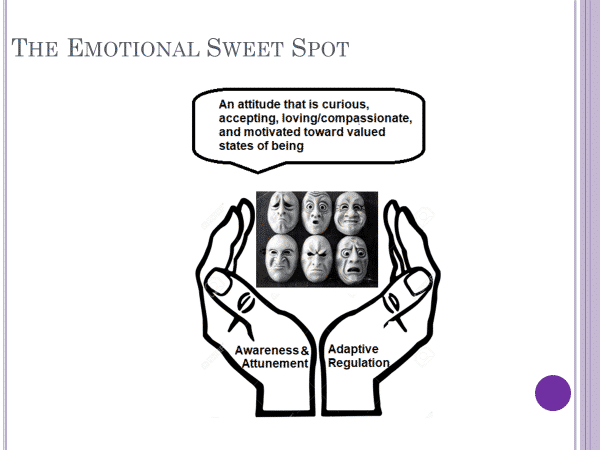
Later, in the back half of this series, we will be exploring different ways for you to relate to your primary feelings and examine how to be aware and attuned to your feelings on the one hand and learn to adaptively regulate them on the other. Here is a diagram to give you a sense of where we are headed.
Our journey of awareness and acceptance continues tomorrow. Our focus will shift a bit and we will broaden the picture. Specifically, we will start to get a better understanding of your overall psychological well-being, your self-concept, and your strengths. These pieces are key contexts in which to place your depressive feelings.
Here is the next blog in the series (Step 7).
Step 7: Understand Psychological Well-Being And Its Relationship To Depression
The reason is that to understand your depression, you not only need to look at it through the lens of behavioral shutdown, but rather we need to consider the whole of your psychological functioning. By understanding the broader picture of your life, you will be in a better position to recognize the things that might be contributing to your behavioral shutdown and things you can do to find psychological nourishment and pathways toward positive investment.
What is psychological well-being?
A good short description was given by the philosopher Immanuel Kant, who described it as “happiness with the worthiness to be happy.”
As this definition suggests, well-being is made up of subjective feelings of satisfaction, contentment and joy (and the relative absence of suffering) coupled with a judgment that such feelings are “worthy” of that happiness. Worth here is generally determined by taking an objective look at the person’s life and evaluating it in terms of functional and moral standards.
For our purposes, if you are engaged in a constructive life and feel good about it, then you have high well-being. However, if you feel you are failing and are not at all being productive in a meaningful way and are having difficulties functioning and are miserable about it, then you have low well-being.
As this description suggests, depression is definitely related to well-being. Generally speaking, if someone is high in depression, they will be low in psychological well-being. However, the point of this blog is to help you see that these two concepts are definitely not the same, and it is important that you have clear notions about both of them.
Some people struggle with depression even as they report relatively high levels of well-being in other areas. For example, the famous psychologist Jordan Peterson has reported that he struggles with depression. I don’t know him personally, but I could imagine he might be someone who also feels he has high well-being, perhaps even if he feels depressed. In addition, there are also some people who have low psychological well-being but are not depressed.
The bottom line is that the two concepts are related, but they are also different in important ways. And it is important for folks who are depressed to think about their well-being and to understand where they are in their well-being and how the two are (or are not) related in their lives.
Related: 7 Tips To Create Instant Well-Being On A Really Busy Day
Step 7a: Assess your well-being and reflect on it in relationship to your depression
The basic way to assess well-being is to ask how you feel like you are functioning in key domains and how satisfied you are with your life, both overall and in specific domains. The “overall” is the assessment someone makes when they are asked how their life is going in general.
Then we look at more specific domains of functioning. For example, how is your biological health and fitness? Are you free from major illness and injury? Are you able to exercise and feel comfortable and confident in your body? Or do you struggle with pain or other health-related problems?
Another key area refers to how you are doing psychologically “on the inside.” This relates to your sense of emotional health, your levels of self-acceptance and your sense of autonomy. Folks who struggle with neurotic loops report low emotional health and low levels of self-acceptance. Autonomy is the sense that you are free from others and can determine your own life.
We can then look more at how you are doing in relationship to your environment. Relationships with others are really key. Do you have high-quality relations with others, or are you alone and isolated? Have you lost cherished relationships? Also crucial is how you are doing at school or in your job or career? And do you have the mental and material resources to control your environment enough to feel secure or does it feel like life is overwhelming you and you can’t cope with all the stressors that are coming at you?
Finally, there is your higher-order sense of being. Do you feel like you are growing and learning? Do you feel like you are developing in a positive direction? And are you able to make deep meaning out of your life? Do you have a philosophy of living or a spiritual sense of your place in the universe that helps guide you? Or are you experiencing a crisis of meaning and perhaps feel that nothing matters?
The point of these questions is to get you seeing the connection (or not) between these domains and your depressive condition. To help advance this understanding, here is a link to a blog that gives you a quick assessment of your overall well-being.
It covers the following 10 areas:
1) Overall life satisfaction;
2) Mastery and control over environment;
3) Emotional health;
4) Relationships;
5) Autonomy;
6) Self-acceptance;
7) Academic (or occupational) functioning;
8) Health and Fitness;
9) Meaning and Purpose; and
10) Personal Growth.
By taking it, you can see where you fall overall, and you can see if there are some domains of functioning and nourishment that are likely connected to your feeling depressed.
As we did in Part IV when we had you take the assessment and reflect on your symptoms, notice the pattern of your scores, relative to your overall score. Specifically, note if there are some areas that you are doing better than in others. How does your overall life satisfaction correspond with your levels of depression? If you score very low on the overall measure (i.e., in adding all the scores, you were below a 30), then it is likely that your depression is tied up with your general living circumstances and how you currently feel about, well, everything.
Related: Ryff’s Model of Psychological Well-being: How Happy Are You?
That is a different profile than someone who is happier overall and has good relationships and good functioning at work or school but struggles deeply with self-acceptance and emotional health. Or maybe you score in the somewhat high range on most domains, but very low on meaning and personal growth. That would say that you feel stuck and are struggling whether your life has the sense of meaning you sense it might (or you are struggling with nihilism, which means the sense that your life is meaningless).

The take-home message for today’s blog is to shift the focus from understanding depression to understanding psychological well-being. The two are related in that as one’s depression gets worse, psychological well-being will inevitably go down. However, the two concepts are not the same.
As we know from this series, depression is a state of behavioral shutdown, where one’s positive mental energy shifts toward the negative. As we have learned today, well-being is about being happy and functioning well in the world across a number of key domains and having a sense of purpose and connection to others. By engaging in a self-assessment you can start to wonder about the relationship between your depression and your well-being. This can perhaps open up new possibilities to guide you, especially when we shift into ideas where you engage in more active change strategies.
This concludes the first half of the series. The next installment (step 8) can be found below. In it, we move to the back half, where our primary focus shifts from Awareness and Acceptance to more Active change principles.
By Active Change, I mean that we are ready to cultivate the part of you that is looking to do something different. Perhaps you might be able to say something like:
“What I have been doing has not been working great for me. For the benefit of my future self, I am willing to try some new things. It will take time and effort, and the effects will not necessarily be immediate. But if I effectively orient myself toward learning and growing and seeking and approaching ‘the good’ rather than avoiding, defending and withdrawing from ‘the bad,’ then I will significantly increase the likelihood I will find a path out of the darkness.”
Step 8 – Values Clarification
To begin this part 8 of the series, we start with a well-known concept in psychotherapy called the stages of change perspective. This refers to the idea that, when it comes to making active changes in their lives, people operate in very different spaces.
Stages of change
Specifically, five different stages of change have been identified. They are:
1. Precontemplative, which means the person is not even conscious of there being a problem and thus is in no place to take steps to change anything;
2. Contemplative, which means that the person is aware that there is a problem and is thinking about doing something, but has not committed;
3. Preparation, which means that the person is getting ready to act;
4. Action, which is when the person is actually trying to do things differently;
5. Maintenance, which is when the person is working to maintain goals at the new, more adaptive level of functioning. When and if someone relapses, they might then return to an earlier phase in the cycle.
By clicking on these blogs, you have demonstrated that you are (at least) in the contemplative stage. And if you have followed along and were waiting for us to get to the Active change stage, then you are in the “preparation” phase. Maybe you have even engaged in some additional reflections from the blogs. For example, if you have tried to internalize things like curiosity and acceptance after reading the blogs, then you already have engaged in some action.
And that is where we are now in the series. We are getting ready to explicitly make the jump into action. The frame that we will be using to guide our general approach is what I call the “adaptive living equation.” As this blog notes, the adaptive living equation means that you realistically try to maximize valued states of being, given who you are and the situation you find yourself in.
Related: Toxic Core Beliefs: 9 Ways To Transmute Them
What do I mean by “valued states of being”? Valued states of being referred to your desired outcomes in the short and long term, based on what you value and your overall situation. Put in the form of a question: Given your values, how would you want to handle the current situation, and what are your desired outcomes in the short term and over the long term?
Here we can build off of our idea of depressive disorders as often stemming from maladaptive patterns of the shutdown. In contrast to adaptive living, maladaptive living refers to ways of being that result in distress and dysfunction and move us away from valued states of being. As we know from our blog series, because of its paradox of shutdown and paradox of effort, depression often gets folks trapped into maladaptive cycles.
As has been discussed, this cycle often involves: (a) an individual who feels highly stressed and vulnerable who (b) hates feeling that way, and (c) is in a stressful situation that elicits negative feelings which (d) causes them to avoid and withdraw which results in them (e) doing less and less (i.e., shutting down) and (f) feeling worse and worse, completing the cycle. Given this, the key is to break the cycle of avoidance, withdrawal, and shutdown, and to find the path to a freer, more fulfilling adaptive lifestyle.
Principle 1 Of Active Change: Values Clarification
Today’s blog is about actively engaging in values clarification. Values clarification involves reflecting on questions such as: What is truly important to you? What moral/ethical/religious system guides your life? How do you make meaning out of the world? What do you really enjoy? What truly nourishes your soul? How do you do what you can to live more in accordance with your values?
Let’s acknowledge that these questions are hard to think about when you are depressed. They take mental energy, which is in short supply. In addition, they might make you start to feel negative feelings because such questions might start to remind you that your life is not where you hoped it would be. Thus, let’s acknowledge that maybe a part of you wants to turn away from this.
However, we should then pause and see that as part of the pattern of the shutdown. You get triggered, you get a jolt of negative pain, and then you move to avoid and escape. This “Trigger Response to pain Avoidance Pattern” is called a “TRAP”, and it is part of what drives folks to shut down. In the next blog, we will get into TRAPs and understand more directly how to avoid them and stay actively engaged.
Today, though, we are interested in values. So, let’s give you a chance to lean in. Here is a 6-minute video on Values Clarification by Dr. Richard Harvey that has some good information. At the very least, take the time to watch that and reflect on it. Ideally, that will lead to you taking the time and doing something more active.
Related: Which Eastern Religion Matches Closest To Your Values? Quiz
For example, here is an exercise on values clarification from Smart Recovery that might be useful. If you are interested in a longer, workbook format, here is a link to worksheets from Acceptance and Commitment Therapy, which is a therapy program and philosophy I find to be quite effective and that overlaps greatly with the view that guides this blog series. Another option is to Google “values clarification” for yourself and sees what pops up.
Today or in the next couple of days, please engage in some form of values clarification and start to think about how you might move yourself toward more adaptive living.
What follows over the next seven entries are seven more key principles for living with depression and for moving toward more adaptive living. They will center on the following domains:
1. Fostering activation and engagement instead of avoidance and shutdown
2. Developing “anti-depressant” habits and lifestyles
3. Fostering a healthy biology
4. Understanding how to engage in the adaptive processing of emotions
5. Developing positive ways of relating to others (and the model of others in your mind)
6. Engaging in more effective ways of thinking adaptively
7. Developing a mindful way of living that fosters growth and adaptive responses to stress

Notice that they are “principles” as opposed to “steps,” which was the language of the first half of the series. The reason is that each principle represents an area of adaptive focus. The blog series is designed to first help you with awareness and acceptance through a series of steps, and then give you tools to foster adaptive living in key areas via key principles. The principles are described and then resources in the form of books, links, and blogs are offered to guide you in furthering the principle in your life in a healthy way.
The word “healthy” here refers to engaging in processes that foster more adaptive living and valued states of being. It is attempting to be in a way that fills one’s souls and the souls of the people around them.
Be aware that each of the principles described below is relatively easy to state, but they are not easy to accomplish, for anyone. They are especially difficult when one is depressed. Consider that a number of them recommend books. Of course, reading books takes effort and time. That is the nature of the game we are playing.
Related: 30 Morning Affirmations To Boost Your Confidence Daily
If you are skeptical of books, be aware that systematic research has found that when folks are in the right stage of change, good books can be very effective in helping guide people out of depressive caves (see here and here for literature reviews demonstrating positive effects that are as strong or almost as strong as psychotherapy or other treatments considered effective).

As has been noted several times in this series, the journey outside the cave of depression can be a long one, and it takes effort and practice. That is true of each of these principles. They are offered for you to consider and they represent some of the ideas that professionals have developed that have good logic and have been shown to work.
However, they only “work” when the individual approaches them with a mindset that is open and oriented toward investing and learning more. Each “principle” can be adopted as the primary focus for one’s attitude and emphasis for change, or you can try to engage in several.
In getting prepared to take more action, I would also like you to remember the “beast” metaphor from the first blog. These principles are not about “forcing” depression out of you (i.e., winning a tug of war and dragging it into the pit).
Rather, each principle involves “seeing” that the beast of depression is there and working to move toward adaptive ways of being even as one experiences its burden. As noted by Acceptance and Commitment therapists, it is possible to both accept the pain one is in and commit to work toward valued goal states.
In the next step in this guide we will explore the core principle of activation and recommend principles for fostering adaptive engagement.
Step 9 : Behavioral Activation (BA)
BA is about deliberately working toward ways you can reverse cycles of avoidance and become more positively engaged in the world around you. This likely sounds pretty obvious (which in some ways it is), but we should note it is not necessarily easy to do. In step 8, we mentioned a way to frame the pattern of shutdown via the acronym “T R A P”, which is an acronym for Trigger, Response, and Avoidance Pattern. We want to avoid TRAPs and engage in positive activation.

Let me translate what this means: A stressor (either outside your head like someone criticizing you, or inside your head, like a scary thought or image) hits your consciousness. That “trigger” results in a painful “response” and that gets you to act via an “avoidance pattern” to be safe. An example can help illustrate what I mean: Joan wakes up and starts imagining her day and thinks about going to work and then being criticized by her boss about something she did. This image becomes a “Trigger” and the emotional “Response” in Joan’s head is a jolt of fear, pain, and resentment.
That makes her want to hide and stay in bed, which is the “Avoidance Pattern”. It is a classic depressive TRAP. To see why let’s play it out. If Joan responds this way, what will the consequence be? If she calls in sick and then lies in bed, where is she but sitting in the cave of depression? Not only that, she still has to wonder if her boss is going to critique her and now she has missed more time from work, so she is further behind.
And it would be likely that she now feels ineffective and has nothing productive to do. That is the nightmare of depressive cycles. The spiral you into the cave. Via avoidance, Joan tried to escape the pain. But her instinct to avoid actually caused her to jump out of the pan and right into the fire.
Related: Understanding your Emotional Command Systems
What should Joan have done?
Ideally, she would have mindfully “held” her feelings, then she would have worked to think things through constructively, and then she would have guided herself to act in a way that was consistent with BA.
In future blogs, we will explore how to think adaptively and mindfully hold one’s feelings. Today our focus is on diving into BA. At its core, BA is about deliberately working to construct one’s way of being in the world that increases engagement, pleasure, and productivity. Over time, this produces what is called a “virtuous growth cycle,” as opposed to the destructive cycle of a shutdown.
More specifically, BA is about finding pathways of positive investment that:
(a) move a person toward specific goals and thus more valued ways of being;
(b) result in mastery, competence, or achievement and the experience of growing and learning; and/or
(c) are pleasurable or entertaining. For a depressed individual, this may well sound both simple and unhelpful.
I can hear folks responding with the thought: “If my life was like that, then I would not be depressed!” We can acknowledge this initial negative reaction. In holding it, it does not follow that we need to give in to the avoidance pattern that follows from it (i.e., the conclusion being that there is nothing that can be done). Instead, the philosophy of BA is an attitude that fosters working toward positive investment.
How does one actually do this? There are many guides for how to accomplish this. Here is a good presentation on the basics of Behavioral Activation. I recommend you spend some time with it (or something similar–feel free to Google “behavioral activation” and look around). As is noted in the guide, BA includes a number of elements, such as
1) Understanding the “vicious cycles” of depression;
2) Identifying goals and values;
3) Monitoring daily activities;
4) Building an upward spiral of motivation and energy through pleasure and mastery;
5) Activity Scheduling;
6) Problem-solving around potential barriers to activation;
7) Working to reverse TRAPs, and
8) Maintaining an attitude that fosters learning and growth.
The guide also includes a detailed description of things like goals, values, mastery, and pleasure, ways to engage in activity scheduling, and ways to identify your core values and goals. It also provides lists of the kinds of activities that many people who are depressed find pleasurable. And it suggests ways to “experiment,” and see which ones are the best for you.
Let me add a few things to the model of BA that they offer.
Model of Behavioral Activation
First, let me note what I call the problem of initiation.
One of the things depressed moods do is “kill” behavioral initiation. This means that, for many depressed folks, it is really hard to get started on new activities. If you are one of these people, I encourage you to employ what I call the five-minute rule.
This is when you make an agreement with yourself that you do the activity for five minutes. Once folks get started and past the initial “inertia” of the shutdown, then they find that the activity takes on a better emotional tone. For example, I am not a huge fan of exercising. And, often, on my ride home from work, a little voice inside my head invites me to keep on driving past the gym, often with some excuse, like it has been a stressful day. My reply to myself is often something like, “Yes, I do feel like crap today for good reason.
So, I will go to the gym and start my workout. If, after five minutes, I still feel like crap, then I will give myself permission to head out.” Usually, five minutes into my workout, I am in a different place and it is much easier to finish it up and by the time I am done, I am glad I did it and feel a sense of accomplishment.
The second idea I would offer is what I call the pay it forward principle.
This refers to the fact that your future self will benefit if you are able to manage to engage in constructive action. Recall the example of Joan. Because she did not deal with the problem, her “future self” now had more problems to deal with. This means hard things built up.
If she had gotten out of bed, and faced the situation effectively–even if she felt miserable during that day–she likely would have woken up the next morning feeling as though she accomplished something. If you have a productive day even if you are not feeling it when it is happening, your future self will likely feel it–just as if you have an unproductive day, your future self will feel that in the opposite way.
I also recommend that in your work on fostering greater BA, try to be clear as to why you are doing what you are doing in terms of your values. For example, if you are cleaning your room, focus on the goal and the fact that doing it moves you to a valued outcome, rather than the thought that you hate dusting or doing laundry. It might help if you think of this as a kind of “behavioral engineering”. You are working to act in your daily life so that it is more engaging, rewarding and leads to greater levels of mastery, goal accomplishment, and pleasure.
In the next blog, we continue with this theme of BA, only there we will focus more on how to construct healthy daily habits and lifestyles. One way to bridge this blog to the next one is to focus on activity scheduling. Activity scheduling refers to the way you plan out what you are doing. I recommend a weekly planner that gives a basic structure to the week. I also recommend a daily planner.
The daily planner is something you do either in the morning when you get up or the night before. It lists the basic tasks and activities for the day. So, today, when I got up, I generated my task list, which included finishing and posting this blog, doing laundry, mowing the lawn, and taking my car to get its oil changed.
It is hard for me to overstate how important BA is to reversing depressive cycles. A good case can be made that BA has more scientific support for treating depressive conditions than any other principle. Of course, if we consider depression as a state of behavioral shutdown, the logic makes good sense. We must also note here that to be successful in employing BA, you will need to learn it and practice it and grow from it.
Related: Why We Need To Be Curious About Mental Illness
As with all the principles that follow, this takes time and effort. And it involves learning at the levels of a) thinking and understanding (i.e., knowing what shutdown and activation are at deeper levels); b) feeling (feeling both the shutdown and the hope and commitment to try to reverse it and feeling the consequences of both), and c) doing (genuinely trying new things and learning from them and adjusting and working to find what is rewarding for you).
This all takes time. This blog gives an outline, but I recommend you seriously “sit” with these ideas and consider really committing to them. To do so you need to immerse yourself in them. There are several excellent books that guide you through this “BA engineering” process. Two such books are:
We have now covered two core principles of Active change. In the previous blog, we covered values clarification and here that of BA. In the step 10, we expand the BAprinciple from a general way of responding to a way of cultivating a particular kind of lifestyle. I look forward to continuing on this journey with you.
Step 10: Healthy Lifestyles
Our primary guide for this part of the blog series is the work by Dr. Steve Iliardi and his excellent book called The Depression Cure (here is a pdf). It starts with the argument that there is a depression epidemic that is spreading, and the likely reason is because our lifestyles. He reviews research findings that suggest that people who life more traditional indigenous hunter-gatherer type lifestyles are much less likely to get depressed. He writes:
Modern-day hunter-gatherer bands—such as the Kaluli people of the New Guinea highlands—have been assessed by Western researchers for the presence of mental illness. Remarkably, clinical depression is almost completely nonexistent among such groups, whose way of life is similar to that of our remote ancestors.
Despite living very hard lives—with none of the material comforts or medical advances we take for granted—they’re largely immune to the plague of depressive illness that we see ruining lives all around us. In perhaps the most telling example, anthropologist Edward Schieffelin lived among the Kaluli for nearly a decade and carefully interviewed over two thousand men, women, and children regarding their experience of grief and depression; he found only one person who came close to meeting our full diagnostic criteria for depressive illness.
What is going on here?
One strong line of thinking is called the “evolutionary mismatch” argument. It refers to the fact that there is a contrast between our current lifestyles and the environment our minds and bodies evolved to live in. Consider, for example, a likely reason we experience tooth decay is that we eat very different kinds of foods than our ancestors.
The same may apply to depression. The lives of our ancestors were, like the Kaluli peoples, close-knit hunter-gather tribes that would live and work together to meet the challenges of survival and reproduction in natural environments. In contrast, we live in a highly fractured, complicated, stressful, high-paced life. Moreover, we can become easily socially isolated in ways that our ancestors would not. This huge difference likely creates lots of problems with our biological and mental health and it provides a good way to understand the modern epidemic of depression.
Dr. Ilardi’s book details a Therapeutic Lifestyle Change (TLC) program that systematically reviews key domains of living and guides the reader in developing healthy, “anti-depressant” habits in each. This is a well-researched program found the following: “Patients were randomly assigned to receive either TLC or treatment-as-usual in the community (mostly medication), and fewer than 25% of those in community-based treatment got better. But the response rate among TLC patients was over three times higher.
In fact, every single patient who put the full program into practice got better, even though most had already failed to get well on antidepressant medications.” The reviews the book receives are generally outstanding. As such, it serves as our guide for today’s key adaptive principle, which is cultivating an adaptive lifestyle.
Six Key Lifestyle Domains
The TLC program identifies six key lifestyle domains, each of which represent areas that our ancestors engaged in dramatically different ways of being than we do.
1. The first domain he identifies is dietary, specifically the consumption of omega 3 fatty acids.
He notes how crucial such fatty acids are for brain function and that hunter gatherers ate much more fatty acid rich foods than we tend to do. He offers a systematic way to monitor and change one’s diet to increase fatty acid consumption.
Related: 6 Ways Food Impacts Your Mental Health
2. The second domain is exercise.
Noting that hunter-gatherers were in much better shape than we are, he encourages physical exercise. I would especially encourage folks to consider walking. Walking with a friend or walking in nature or walking while you listen to music or a podcast on a topic you are fascinated by is a great way to get exercise and also make connections and be outside and learn new things.

3. Productive engagement
Much as our previous blog, Dr. Ilardi emphasizes the need for productive engagement with various activities and explores ways to foster such engagement in one’s life.
4. Sunlight exposure
We spend much of our time indoors and are exposed to natural sunlight much less than our ancestors. We know that light therapy is important for bipolar conditions and Dr. Ilardi argues that sunlight exposure is helpful for our bodies and minds to feel alive and engaged. The book recommends increasing sunlight exposure and provides clever ways to accomplish that.

5. Social support and connection is the fifth lifestyle.
In a future blog entry, I will be discussing the importance of relationships and feeling secure and known and valued by others. Here we can note the importance of human connection and the book examines ways one might increase connection with others. For example, one might join a club or a church or invite a friend to become a regular walking partner.
Related: How Emotional Support Animals can Help with Mental Health
6. Sleep

Sleep is one of our most important habits and a regular and fulfilling sleep pattern is crucial for our health. The book explores good sleep hygiene and offers suggestions for getting a good night’s sleep.

Dr. Ilardi’s Depression Cure is an excellent resource to foster an “anti-depressant” lifestyle and I highly recommend it. Whereas behavioral activation serves as the basic adaptive principle, the lifestyle approach provides a systematic guide toward constructing a life that is more robust and resistant to depressive cycles and shutdowns.
Let me conclude this blog with two other books are work considering. Spark is a book on the benefits of exercise and getting more physically active and Go Wild is a more recent book by the same author on living a more natural lifestyle can foster well-being. In the next blog, we turn our attention to the biology of depression.
Step 11: Taking Care Of Your Biology
Let’s divide your “lifeworld” into three domains.
The first domain is the personal domain
which is the self-conscious part of you.
This is part of you that is reading this blog and deciding what it means.
Related: Self-Care 101: What do Self-Help Ideologies Have In Common?
The second domain is the mental domain.
The mental domain consists of your sensory inputs, motor outputs, and feelings and drives and other subconscious processes. These are “sub-personal” in that they connect to the personal domain, but they are not as directly controllable as the personal domain.
For example, you can personally decide to stop reading this blog, but you cannot decide to “not see” the visual input that comes to you when you open your eyes.

Finally, there is the impersonal biological part of you.
Your heart is pumping, your blood is flowing, your brain’s neurons are making new connections. This is the domain of biology. These things “just happen” and you have no direct knowledge of them, nor do you have direct control over them (although see below). That is what makes them “impersonal.”
I have introduced these three categories of personal, mental and biological to help clarify the potentially confusing relationships between “biology,” “disease,” and “depression.” When folks think about depression as a kind of disease, they have in mind the idea that the cause of the behavioral shutdown stems from something that has broken or malfunctioned in that domain. Consider, for example, the “chemical imbalance” hypothesis for explaining depression. This is the idea that depression is caused by problems with neurotransmitters, the special chemicals that foster communication between neurons in the brain.
Many people think about depression as a kind disease. Is this wise?
This blog series encourages you to think about depression as “biological” (as well as mental and personal) but to be cautious about thinking about it as a “disease.” To understand why we should be cautious, we need to understand the research-based reasons and the psychological reasons.
The research-based reasons are simple: for many, many years, Western medicine has looked for disease-type mechanisms and faulty genes that try to explain the underlying cause of depression in terms of broken biology. The result of all this effort can be summarized as a complicated mishmash of findings and no clear result.
The “chemical imbalance” hypothesis, for example, is almost certainly wrong. In addition, the thousands of studies looking for specific genes for depression have basically “struck out” and failed to find anything definitive. More recent neuroscience research is examining the “inflammation” hypothesis. Perhaps that will yield something of use, but as of now, unless you want to become an expert in neuroscience or psychiatry, then there is not much information on “depression as biological disease” that is helpful.
The psychological reason to be cautious about the “depression as disease” idea is because of what the idea justifies. The key thing here is that it offers an “impersonal justification” for one’s depression, which has some potential benefits but also a number of costs.
Consider that if depression is caused by faulty serotonin production, then it follows that the person (or the family or life circumstances) are surely not at all responsible for the sad state of affairs. We can see this when we move to more traditional disease states. For example, when I got a rare cyst in my spine, no one asked me about my self-esteem or my relationship with my mother—the cyst was obviously caused by an impersonal, biological malfunction. Likewise, if depression is caused by impersonal biological breakdowns, then it follows that folks are relieved from all personal responsibility.
Because of this consequence, the justification can feel good and may even be helpful in some cases. It is the case that many people who are depressed are prone to excessive self-blame and so relieving some personal responsibility can be helpful. (Note that research has looked at the impact of thinking of depression this way, and the results are mixed).
But it is also the case that this justification can work in highly problematic ways. Most notably, it can function as a psychological defense against looking at one’s life, one’s relationships, one’s coping styles, one’s emotions, and one’s personal narrative for living. This can be a real problem.
At a broad societal level, the idea that depression is primarily a disease is almost certainly problematic. The unified theory of psychology approach that I developed states we should consider depression a state of behavioral shutdown. This means that the appropriate “placement” of depression is to consider it as a mental phenomenon.
Because the mental domain lines up with the domain of behavioral activity, it means that the primary intervention of behavioral activation (described here, in the ninth step) deals with depression at the right dimension of analysis.
Even if we locate it primarily in the mental sphere, depression clearly involves both the personal and the biological domains. This is not surprising because these three domains are all interconnected. Consider that you are engaging with these posts at the personal level.
That is, you are choosing to read about them, think about them, and following the advice they offer (or not). If they help you, it is because they have altered your self-conscious understanding of depression and that has impacted what you have done and felt.
To see how the domains are constantly interacting, let’s take a moment to engage in a brief exercise:
First, breath gently through your nose for a period of 10 seconds.
Second, engage in a relaxed “soft gaze.”
This is where you allow your vision to stare at some ill-defined figure, like the corner of a table, and you gently attend to the periphery of your gaze. Do that for 10 seconds.
Finally, breathe such that you inhale through your nose and then engage in an extended exhale, for 10 or so seconds, pausing for two seconds prior to inhaling again.
Do that for 10 breaths.
If you have taken the time to do this, you almost certainly altered your biology. The reason is that engaging in this activity alters the behavior of your vagus nerve, which is a highway that connects the brain to many parts of the body. This kind of breathing also changes the ratio of activation in your sympathetic and parasympathetic nervous system, moving you into a more relaxed, parasympathetic state.
The idea here is something that you already know intuitively, which is that how you personally direct yourself impacts your mental states and your biological states. Thus, although you don’t have direct control over the impersonal biological domain, you clearly have indirect control over much of it.
A key aspect of depression is taking care of your biological domain. This involves learning how to harmonize your personal, mental, and biological dimensions of being. The breathing exercise provided you a glimpse into how you might systematically create “flow” and “harmony” between your personal, mental and biological domains. This is a window into the world of meditation, which I think depressed folks should seriously consider.
A previous blog post on healthy lifestyles provided information on key habits, like eating, sleeping, and exercise. The adaptive principle of living in this post is the idea that the body is the “temple” in which your mental and personal domains reside. To help with depression, it is crucial to listen to what your temple is telling you and to try to take care of it accordingly.
For some resources that might help guide you in taking care of your body and its chemistry, consider the book Depression Free, Naturally, which outlines a seven-week “emotional healing” program that emphasizes diet, nutrition and body chemistry. Another potentially useful book is The Chemistry of Joy (and accompanying workbook). This book guides you toward understanding your depression and provides a specific lifestyle plan to address it, as well as nutritional supplements and mindfulness exercises that the author’s claim can restore your body’s natural balance and energy.
This concludes our 11th entry in the series. Next time we dive fully into the domain of emotions, where we will explore how to relate to emotional reactions and hold them in the “adaptive sweet spot” of the mind, where one is able to be aware and attuned to them on one hand and able to adaptively regulate them on the other.
Step 12: Relating To Your Emotions
This entry is about emotions and learning how to process them adaptively. We explore what emotions are, why emotional awareness and regulation are key skills, and briefly describe how to hold emotions in what I call the Emotional Sweet Spot.
Emotions are a key aspect of depression, and many depressive episodes emerge from conflicts people have with their feelings, which is why so many psychotherapies are “emotion focused.” What, exactly, are emotions? Emotions are “perceptual response sets,” which means they are activated by an appraisal of an important event and orient the body, mind, and self-consciousness system to respond accordingly.
This means there is a physiological component to emotion (e.g., your body will become aroused or disengaged), an experiential component (e.g., you will feel either positive or negative and orient to move either towards or away from certain stimuli) and a narrative component (i.e., you will be more inclined to think about a situation in a particular way when emotion is activated).
Related: 12 Signs You’re Uncomfortable With Emotions and How To Accept Them
Classic or core emotions represent evolved “signatures” for perceiving and responding to the world. As was seen in full display when the US women’s soccer team won the World Cup, joy is activated when one receives feedback that one’s goals or desires are or will be met. Anger is another classic signature emotion. As this experiment with monkeys demonstrates, anger is activated when an individual perceives their rights or interests have been violated or they are treated unfairly. Sadness, fear, guilt, shame, pride, love and hate are all-important emotional states. Because it is helpful to have a rich emotional vocabulary, here is a list of emotion-related words.
Emotions are centered in the domain of the mental. This gives rise to a second key point, which is that conflicts often arise between the mental and personal domains of one’s lifeworld. Let me disclose a personal example. There was a period in my life when I had real problems processing sadness, such that I went almost 15 years without crying. As soon as I would start to feel sad, I would feel helpless and vulnerable in a way that was not consistent with how I wanted to see myself as a man.
The conflict between my personal domain and my emotional domain created a disharmony that resulted in some limitations and blind spots. I recall when I tapped into these feelings, I was flooded with tears and injuries that I had been blocking for a long time. The point here is that we humans have both primary emotional reactions and then secondary emotional reactions (and other coping tendencies) to those primary reactions. In the clinic room, we see that much mental distress is about “affect avoidance,” which is the technical term for inhibiting or blocking key feelings.
In an earlier blog in this series, we explored the concept of “neurotic loops.” A neurotic loop is when an individual has secondary negative reactions to negative feelings, which creates inner conflict and distress. This disrupts the natural flow of the emotional system and leaves people feeling all tangled up inside. This is important because the consequence of such emotional tangles is often a depressive shutdown.
What does this mean for you and your depression? It means you should be aware that there are healthy and unhealthy ways of relating to your feeling system. The unhealthy way, described in the neurotic loops model, is by trying to block, control, attack, or avoid one’s core feelings. The healthy way is via cultivating a different relationship with one’s feelings, what I call the Emotional Sweet Spot (ESS) model. It starts with a couple of key insights.
Related: The Shortest Ultimate Guide To Dealing With Emotions
Emoitional Sweet Spot
The ESS starts with the idea that we have feelings for a reason and they are a vital aspect of our lives. They teach us about our core, embodied values and how things are going in our life and it is crucial that we integrate them into our being to be fully human. However, it makes good sense as to why internal conflict arises in relation to emotions. Some of the key reasons are that (a) negative feelings suck, and (b) they often remind us of painful wounds that we can’t do anything about, and (c) they activate impulses that can be problematic.
These two insights are, of course, somewhat contradictory. This means that we humans have much to learn regarding the complicated process of dealing adaptively with our emotions. Unfortunately, our society is not good at teaching emotional intelligence and so many people get confused and all tangled up for a host of reasons. (Consider that, throughout their elementary, middle, and high school years, my kids were never taught anything about emotions).
According to the ESS model, the healthy way to relate to one’s feelings is to be (a) aware and attuned to one’s feelings on the one hand and be able to (b) adaptively regulate one’s feelings in accordance with one’s short- and long-term goals on the other.
Here is a diagram that captures this model. It also involves changing the attitude from the inner critic. Instead of being critical and controlling or avoiding of feelings, as the neurotic loop model highlights, the attitude one attempts to cultivate is one of curiosity, acceptance, loving compassion, and motivated toward valued states of being.
How does one accomplish this?
It is a process that requires both intellectual understanding, as well as courage, and practice. In addition, human emotions are very relational, and so ideally it takes place in a particular kind of relationship that is safe and secure.
The most basic process starts with an awareness of the conflict between the head and heart.
Specifically, this involves questions such as: How connected am I to my feelings?
What feelings are hard for me to feel? What makes them hard? These are “awareness” type questions, fostered by the attitude of curiosity, which we discussed in this blog.
Second, there is the capacity to accept the emotions one has.
This is hard and can be extremely difficult in distressing and threatening environments. Meditation and other distress tolerance models have been developed to help folks learn how to maintain a presence in the face of pain.
Third, is the capacity to integrate the feelings while maintaining clarity about one’s goals and values in the short and long term.
This means being aware of the outcome one desires and channelling the responses energized by the emotion into adaptive ways.
For example, if someone experiences road rage, the key is to help learn what the anger is about, what it comes from, but also be able to recognize that impulsive, aggressive responses are maladaptive and need to be effectively regulated.
Below are some additional resources for learning to cultivate your capacity to hold emotions in the sweet spot between awareness and attunement and adaptive regulation. One final comment I would like to make is a distinction between an emotion and a mood. The former is a charged reaction to a particular stimulus. It is something that if it is responded to via the ESS, when you “arrive” at it will integrate your physiology, your mental frame, and your narrative and you will then fairly quickly leave it.
Related: 10 Signs You Are Emotionally Wounded
That is, peak emotions tend to only last seconds into minutes. In contrast, moods are more general states of mind that last hours into weeks or more. Depression is a mood state, and mood states are often things you want acknowledge but counterbalance (i.e., instead of giving into the shutdown mood, get activated).
To start the process of diving in to healthy emotional processing and move from the neurotic loop model to the ESS model of feeling, I have developed this “blog tour” that details a series of steps for learning how to deal with negative feelings via my unified approach.
For a book length treatment on why openness and curiosity are better ways of relating to one’s feelings rather than rejection and escape, I recommend Todd Kashdan’s The Upside to Your Downside. Dealing with grief and loss are particularly important emotions associated with depression. The book Progressing Through Grief: Guided Exercises to Understand Your Emotions and Recover from Loss by Stephanie Jose provides a helpful guide in processing grief.
By far the most common and powerful emotions we tend to experience are relational in nature and are activated in response to our core psychosocial need to be known and valued by important others in our lives. In our next entry, we look at the crucial role relationships play in depression.
Step 13: Understanding Relationships That Connect To Depression
In this blog we explore one of the most central human concerns, relationships. Specifically, we examine four kinds relationship problems that connect to depression (i.e., loss, rejection, isolation, and loneliness), and we briefly review attachment and interpersonal styles and conclude with offering some suggested readings on relationships and depression. (See here to start the series).
Few things nourish the human soul more than love. But what is love and why is it so central? According to the unified theory, human beings have a core “relationship system” that guides them in their social worlds. Being loved, in its most general form, refers to the experience of being known and valued by important others—it is one’s felt sense of having relational value (RV).
An important and related variable is social influence (SI), which refers to the extent to which one can move others to act in accordance with one’s interest; it is one’s social resources or social capital.
The human relationship system is centrally organized around relational value and social influence—humans seek both in their exchanges with others. This is called the “RV-SI” line on a map of the human relationship system called the Influence Matrix. This refers to the fact that people will have both a general sense of RV-SI (high or low or somewhere in between), and they will subconsciously track losing or gaining RV-SI in social situations and feel accordingly.
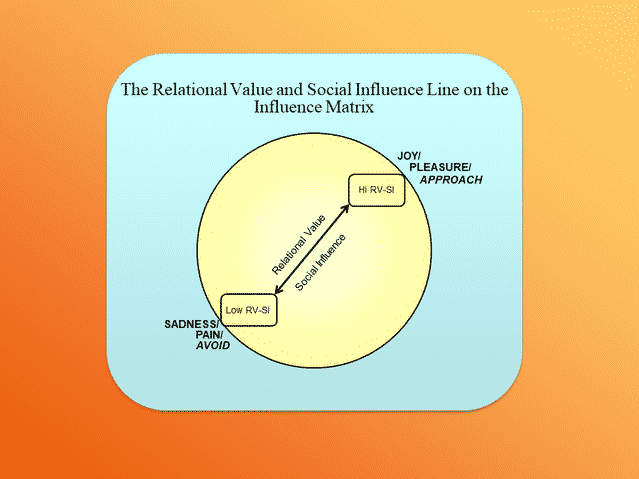
Relational nourishment refers to the extent to which folks have their relational value and social influence needs met across their development.
There are four primary relational domains that we humans track for nourishment:
1) family;
2) friends;
3) lovers, and
4) groups or communities we belong to.
Thus to understand a person’s relationship system and status it is important to reflect on the extent to which a person has felt known and valued across these four areas. We can start with one’s place in one’s family, most notably an infant’s “attachment” to its primary caregivers and then track the other relationships in one’s family of origin. By kindergarten, friends become central, and so has one’s place in the peer group and a larger sense of belonging (or not).
In adolescence into young adulthood, the domain romantic love emerges as key. Problems in these domains set the stage for what might be called “relational malnourishment,” which is one of the key causes of depression.
Related: Why Are On-Off Relationships Harmful For You?
There are four kinds of relational problems people with depression often face.
First, there is the loss of an important other, either via death, dissolution, or other disruptive forces. The loss of the loved one is the focus of Freud’s primary work on depression, Mourning and Meloncholia. Freud argued that individuals long for union with their lost loved ones; this is normal mourning.
However, he argued that some individuals (often unconsciously) cannot get over the loss and end up feeling paralyzed, dejected and rageful about the unfairness of it all. Ultimately, this rage would be subconsciously directed inward, giving rise to a depressive shutdown (melancholia).
Rejection is the experience of being criticized, disrespected, abused, or unwanted. It is a direct attack on the need for relational value and social influence, and thus it is one of the most painful things a person can experience. Chronic rejection is one of the strongest causal predictors of depression.
Social isolation refers to folks who have few opportunities for connection and influence. Thus, a person in a strange land or who made no friends would experience social isolation. It is low social influence situation.
Loneliness is related to social isolation, but it is also different.
It is the felt sense of not being truly known and valued.
Thus, a person might on the surface appear to have lots of connections, but they are wearing a mask and do not feel like they are loved for their true self. This means they are low on their inner sense of relational value.
Given human’s core need to be loved, it is not surprising that loss, rejection, social isolation, and loneliness are all strongly associated with mental pain and depression. What are the implications for depression?
It means that to understand one’s depression, one must wonder about the connection between the mental shutdown and failing to be nourished relationally (i.e., dealing with loss, rejection, isolation or loneliness).
To deepen your understanding of the human relationship system, it is helpful to understand one’s attachment and interpersonal style. Attachment refers to the felt sense of bonding, harmony, and security (or its absence) between individuals.
When infants are born, they are organized to seek a harmonious and secure relationship with significant caretakers. Basically, they want to know that they are known and valued and will be protected if threatened. If they develop a healthy relational dance with their caretaker, they will feel “secure.” If do not feel this, they will develop an insecure attachment style.
There are three major insecure attachment styles that take shape in adolescents and adults.
One style is an “other-oriented, anxious-preoccupied” style that orients the individual to be a bit dependent on others and constantly seeking approval or contact.
A second attachment style is essentially the opposite: a counter dependent, “dismissive” style that downplays relational needs (i.e., if someone says in therapy that they don’t care what other people think or feel about them at all, then they are likely being counter dependent.
Interpersonal style refers to one’s basic tendencies for interacting with others, and it shows up in terms of key personality traits, such as extraversion and agreeableness. When people are forming first impressions, they look for friendly and confident styles of being, and so folks who are low in either extraversion or agreeableness makes it more challenging to develop new relationship connections.
Related: What Does It Mean to Have an Insecure Attachment Style?
Here is a quick, free assessment to get a sense of your level of agreeableness. Attachment and interpersonal styles are often aligned such that there are a number of folks who are agreeable and dependent (other-oriented).
On the flip side, there are others who are both disagreeable and counter dependent/dismissive (self-oriented). Folks who have extreme other-oriented or self-oriented relational styles often experience difficulties getting their needs for relational value and social influence met.
It is also useful to keep in mind that a significant subset of relationship problems stem from being “hypersensitive” or fearful and avoidant in social situations. This refers to a feeling of fear or dread or a massive aversion to conflict or criticism which then causes people to avoid contact. If you think this might describe you, then you should perhaps check out this blog on social anxiety.
Related: 14 Personality Traits of People With A Secure Attachment Style
Although our focus in this blog series is on the individual and structured from a self-help perspective, it is crucial that we are all aware that our society is structured in a way that has many “cracks” for people to fall through.
In an earlier blog in this series, it was noted that depression is virtually unknown in hunter-gatherer societies. We humans are structured to be part of a connected and interdependent band of people that work together on the projects of living. The modern industrial/information age society is much more individual and fractured and fragmented.
It is highly likely that many people are depressed because their core relational needs are going unmet. A recent book by Johann Hari called Lost Connections: Why You Are Depressed and How to Find Hope explores the concept of depression and emphasizes the key is understanding how it emerges from being disconnected. He offers a very engaging and sophisticated look at depression from this perspective and helps people consider ways that they might reconnect with the world in a healthier and more adaptive way. In addition, here are some other books on fostering healthy relationships.
In the world of psychotherapy, there are a host of “interpersonal” approaches to depression.
The focus of interpersonal therapy includes helping people overcome problems with:
(a) transitions into new roles;
(b) grief or loss of old roles;
(c) ongoing conflicts and disputes; and
(d) lacking skills and dealing with heightened interpersonal sensitivity, like shyness.
If you think you need help in understanding your relationship style and the ways that conflicts in a relationship might be central to your state of shutdown, here is a self-help book, called The Interpersonal Solution to Depression. You can buy from here
This blog and the previous one on emotions represents the “mental core” of depression. That is, the “heart” of depression very often centers on relational dynamics and problems of loss, rejection, isolation, and loneliness, coupled with negative emotions that then result in a vicious cycle of problems and ultimate shutdown. The next blog shifts the focus to the “head” and explores ways you can learn to engage in adaptive self-talk.
Step 14: Adaptive Thinking
This entry is about “thinking” and learning about how to think about thinking and what kind of thinking is adaptive versus maladaptive. How you think has a profound impact on how you feel and what you do, and it also influences how situations unfold. In addition, people can actively learn how to catch their thoughts, check them, and change them to be more adaptive.
The “cognitive model of depression” is one of the most well-known models of depression. It was developed by Aaron T. Beck, who is often considered the “father” of cognitive therapy. I am very familiar with it because I worked with him for four years at the University of Pennsylvania (1999-2003).
Cognitive refers to thinking, especially verbal thoughts and what we might call “self-talk,” which refers to how you make sense of things, others, the past, and possible futures. In the language of the unified theory of psychology, this kind of thinking stems from a person’s “justification system” because it is the system of thought that functions to verbally justify what is happening and what ought to be done about it.
The cognitive model points out that how you think about things plays a key role in how you feel and what you do. To see what I mean, let’s imagine Mark is a college student who is feeling depressed and is stressed. When asked how his weekend went, he states:
“It was not great. I couldn’t go to the party I wanted, which sucked because I missed out. Instead, I had to stay home and do homework.”
Notice that Mark’s “justification system” frames the world as acting on him and controlling him through costs and threats of punishment. This suggests he has an “external” locus of control and means he will likely be reactive and defensive in his stance in the world. We can see this if we contrast it to a frame that reflects an “internal” locus of control. For example, imagine if he had said:
“A part of me wanted to go to the party, but I decided it was best if I stayed home and finished my homework since I want to do well in school.”
Related: 7 Negative Mindsets That Undercut Your Mental Strength and Resilience
Here Mark’s system of justification frames his place in the world such that he is an agent and is in much more control of his decisions and is choosing to act based on his values. If things are framed in terms of “I am doing what I am choosing to do because this is the best option for me,” then the emotional system is in more of an “approach” state.
Given our discussions about depression as a state of behavior shutdown, I am sure you can see why framing things defensively and in terms of punishment is much more consistent with shutting down. This means that how you think about and frame your place in the world might play a major role in your mood.
Beck’s cognitive model teaches people to first recognize that interpretations matter for how they feel and what they do. Second, it teaches people to recognize that interpretations of the world are not facts about the world, even though our emotional system treats our interpretations as if they were facts. Let’s imagine Joe is in a depressed and anxious mood state. He gets an email from his boss at work that reads:
Joe, there is a problem with the report you handed in. Can you give me a call?”
Joe’s heart jumps into his throat upon reading this. Immediately his mind goes to all the possible outcomes, virtually all of which are catastrophic. He runs through all the questions that he had when he put the report together and starts envisioning that he made all the wrong choices. He then starts to resent his boss for giving this assignment to him in the first place. He knew he should have refused because he was not in a place where he could handle this assignment.
After an hour of mental torture, Joe finally feels the pressure strong enough to calls his boss. He picks up his phone feeling fearful, defensive, and guilty all at once.
From the cognitive model, we can see how Joe engaged in a massive amount of interpretation based on relatively few facts. The only facts here are that his boss wants to talk to him about a problem with a report. Of course, it is possible that there is a major problem with the report. But it is also possible that the problem is either minor or not even something Joe did. Maybe someone else did something to it that created the problem and the boss wants to problem-solve, rather than blame Joe.
There are a couple of lessons that we can learn from this.
First, interpretations are very different from facts.
Second, we operate much of our lives off of interpretations that carry assumptions that we have filled in.
Beck was fond of saying, “Check your assumptions because if you are wrong, they can make an ass out of u and me.”
Beck’s cognitive model divides the justification system into 3 levels.
The content on the surface of one’s justification system is called one’s “automatic thoughts”.
Automatic thoughts refer to the “ticker tape-like” stream of interpretations that people are constantly making as they narrate things to themselves. They are “automatic” because they often come as habituated forms of interpretation and are not generated with much conscious effort. When people are depressed, their automatic thoughts tend to shift into what Beck called the “negative triad,” which refers to negative thoughts about oneself, one’s future and the world (especially other people). We can see lots negative automatic thinking in Joe.
The next level of thinking Beck identified occurs at the level of inferences or “if… then… conclusions” people draw from bits of information.
Beck noted that many depressed folks make lots of “cognitive errors” in the negative direction. That is, they take ambiguous information and then jump to strongly negative conclusions. I did my dissertation on this concept, showing that people who tended to make negative cognitive inferences felt significantly worse after receiving ambiguous feedback than people who made positive cognitive inferences.
Related: What Is Cognitive Dissonance? Common Causes and How To Resolve It
Here is a list of the kind of negative cognitive errors people who are depressed or anxious tend to make. I recommend learning this list and seeing if you recognize any of these tendencies in your own thinking style.
The deepest level of Beck’s model was “core beliefs”.
These are the core organizing “schema” that frame how someone thinks about themselves and the direction of their lives. Beck argued that depressed people tended to have core beliefs that they were either incompetent or unlovable or both. When folks are not depressed these core beliefs can be dormant. But depression charges these modes of thinking, and then this becomes a basic frame for understanding what is going on.
We can see this with Joe, as he interprets the message as meaning that he likely was not competent to handle the report. If we were to dig a bit deeper, it would not be surprising to see that Joe has struggled to feel competent his whole life and when he gets depressed, he has the experience that he is fundamentally incompetent.
The cognitive approach to depression is a systematic approach that teaches you how to think about your thinking in a more adaptive way. It helps folks realize that interpretations are not facts and that negative interpretations can fuel negative feelings and avoidance and shutdown tendencies. That is, negative thinking can drive you into the neighbourhood of depression. Sometimes absolutist negative thinking can “dead-end” folks so much that they start contemplating suicide as the only solution.
We should note that it is also the case that depressed moods activate tendencies to think in negative, pessimistic and avoidant ways, so there is a vicious cycle here that can feedback on itself. That is why learning about how to think can be so helpful. It helps keep this cycle from spiraling out of control. It is worth noting that thinking has been the focus of self-help books for depression more than any other domain.
Related: Cognitive Defusion: The Unconventional Technique That Helps My Anxiety
Most self-help approaches fall under the heading “cognitive behavioral”. This is because they attend to both behavioral activation principles and help people identify their problematic thought patterns, learn to consider adaptive alternatives, and learn how to replace rigid, or maladaptive thoughts with more adaptive ones.
When I was at Beck’s research lab, we framed the basics of the cognitive model in terms of the three Cs. What we meant by this was that we taught folks how to “Catch it” (i.e., identify the thought), “Check it” (ask whether the thought is accurate and helpful, or not) and if necessary then “Change it” (replace the thought with a more realistic and adaptive interpretation).
So, if we were working with Joe, we would help him “catch” the fact that he was “catastrophizing” (a common cognitive error) and help him evaluate his interpretation and then change it to be more accurate and helpful and frame his situation in a more adaptive way. Ideally, his self-talk would be transformed into something like: “There is a problem, but I don’t know exactly what it is. Before reacting, I should calmly find out what the problem is. If it is my fault, I will need to summon the strength to deal with that maturely. Regardless, I want to try and help fix it to the best of my ability.”
If you are interested in diving into the cognitive approach, here are two excellent book-length resources that many people have found to be valuable. First, Feeling Good: The New Mood Therapy by David Burns is a classic in the field. I think it is the most popular cognitive self-help book ever developed. Another good book that is grounded in a cognitive perspective is Mind Over Mood. It provides readers with strategies that can help them learn to manage their minds, control their negative thoughts, and end for good the distress of depression.
Over the past 15 years or so there has been a debate in the cognitive behavior community about how to relate to one’s thoughts and feelings. Should folks be taught to “catch, check and change” their thoughts as I have argued here? Or is it better for them to learn to become aware, accept them as thoughts, and then just move toward valued goal states without trying to engage and change the thoughts?
The latter is the philosophy of Acceptance and Commitment Therapy (ACT). My professional opinion is that awareness, acceptance and active change are all good ways to go, so I don’t think we need to choose between them. But ACT does provide a different way of learning how to relate to one’s thoughts and feelings. Readers may recall that I used a common ACT metaphor of the “beast” of depression in an earlier blog. I support both the traditional cognitive frame and ACT. Here are two excellent books on depression from an ACT perspective.
Steve Hayes is the founder of ACT and he co-authored the first ACT self-help book in 2005, which was Get Out of Your Mind and Into Your Life. It reviews the basic principles of ACT. Robinson and Strosahl developed more traditional workbook/self-help based on ACT for depression called The Mindfulness and Acceptance Workbook for Depression.
That brings us to a close on how to think adaptively when you are depressed. The next post focuses on identity, defenses and the shadow, and move toward a general philosophy of living. That will be the final official entry in the series.
Step 15: Identity And Shadow Work
This blog focuses on some deeper domains, including reflecting on one’s identity and philosophy of living, defenses and shadow works, and concludes with a general approach to psychological mindfulness. This is our last official entry, although I will offer a final summary of the blog tour summary that includes links to the entire blog series so that in the future folks can just click on one link.
The principles of active change explored in the second half of this series have been focused on pragmatically reversing cycles of shutdown and finding more adaptive ways of being in the world.
This final entry is a bit more abstract, broad, and deep. It focuses on developing your philosophy of living and a fuller understanding of yourself. It is based on the idea that if we are going to truly organize our lives in a way that really allows for a “growth-to-goodness” trajectory, we need a core understanding of our place in the universe, a framework to make sense of right and wrong or to assess valued states of being, and ways of reflecting on things larger than our lives.
Related: Shadow Work: How to Let Your Inner Demons Guide You
This is the moral/ethical, existential, spiritual, and/or religious dimension to living. It deals with questions such as:
What makes human life valuable and worthwhile?
What is our place in the cosmos?
How do we know what kind of life we ought to lead?
What is authentic well-being? What is evil?
Who am I really? And, given that, how should I live my life?
Answering these questions in meaningful ways requires exploration, reflective thought, and searching for systems of meaning that resonate with you. One potentially helpful place to start is here, with the “eulogy” exercise. The eulogy exercise involves thinking about your life’s trajectory having come to the end and looking back on what it meant. It is a perspective that helps folks sort out what really matters in the world. As this entrepreneur notes, facing death can really give one perspective on such things.
In addition to reflecting on one’s own life and values, I think it is crucial to explore the ideas of others.
Victor Frankl’s classic (and short) book, Man’s Search for Meaning, is a great source for thinking about good and evil and how one wants to be in the face of great tragedy.
A more broadly educational source for thinking about meaning is the Great Course titled, The Meaning of Life: Perspectives from the World’s Great Intellectual Traditions. Another potentially useful course focused on developing a deeper understanding of who you are is Jordan Peterson’s self-authoring platform.
The point here: Humans seek meaning in our life world and need it to unfold as a storied “life quest”. As such, we need a broad reference point to make sense of our lives and to know what we are or ought to be headed toward. This is why it is crucial to develop a philosophy of life that informs you about who you are and the kind of life you hope to live. This connects to an earlier post in the series, where we explored your values.
We need to acknowledge that the quest to deeply understand one’s identity is not just about developing a clear set of values and a richer understanding of how you want to be. It also needs to involve what is called “shadow work.”
Related: How To Own Your Shadow Before It Owns You: 7 Helpful Exercises
As is well-known, humans engage in much defensive filtering of information. We filter out the stuff we don’t like to think about and stuff about ourselves we wish was not true. Old wounds, vulnerabilities, areas of low self-esteem, need for power, feelings of resentment, and so on drive much of what we do, even as we deny this to be the case. Shadow work refers to peering behind the filter of self-consciousness and seeing what the subconscious system feels that we are trying to deny.
I have had people say to me: “My depression must be biological because everything in my life is fine.” This framing suggests that they are likely defended against things. Why? Because everyone gets injured or has longings or dark feelings that might contribute to feeling shutdown.
A blanket denial of the possibility of problems is thus suggestive of someone who has not pulled back the veil and looked squarely at the darkness that is much of the human condition.
I recommend that, in addition to exploring one’s identity and values, one should also explore the darker side of one’s psyche. What do I mean by this? The stuff that your self-consciousness system tries to block, deny, repress, or rationalize. These are psychological defenses, and here is a helpful list to familiarize yourself with them.
An implication that we shield our psyches from unwanted or painful thoughts gives rise to the important idea that there is a shadow side to our conscious being. As suggested above, your shadow can be thought of as the part of you that you hope you are not, but fear you might be.
Here is a post on the shadow and dancing with another’s shadow, and here is a video on the shadow. Finally, here is a self-help course that folks can take devoted to understanding your shadow. The shadow is an important psychological concept for you to be aware of and shine some light on.
Diving into the shadow is not recommended for folks in the middle of a moderate-to-severe Major Depressive Episode. The reason should be pretty obvious (folks are already in hell and seeing hell all around them).
However, it can be helpful for folks who struggle with depression and want to explore deeper into their psychic lives. I mention it here at the end of our pragmatic journey out of the cave of depression because I believe that doing shadow work and coming to terms with one’s shadow enables individuals to develop a more robust character and a lifestyle more resilient to depression. Thus, it is an appropriate task to engage in as the system recovers and is in a place to engage in searching and growth.
CALM M.O.: A General Approach to Fostering Mentally Healthy Living
Although the work of finding out who one is at a deeper level can only be done by the individual finding their own path, there are some key principles one can follow. Obviously, the idea of the shadow gives some frame for where to look.
But what about how to look?
During this series, we have repeatedly emphasized the stance of not giving in to the emotional reaction to “avoid and withdraw,” but instead work to override that instinct and try to “seek and approach,” with the goal of finding paths of investment that nourish your soul.
I will leave you with a basic approach to cultivate healthier emotional living, encapsulated in the acronym: CALM M.O. This is structured to offer a quick frame of reference that fosters an integrative approach to psychological mindfulness.
Being mindful means being aware of one’s surroundings and adopting a reflective and accepting stance rather than an automatic or instinctual “mindless” way of reacting or resisting or escaping.
The M.O. stands for two things.
The first is a “Metacognitive Observer,” which means one adopts a reflective, mindful attitude where your mind becomes the object of observation. It also doubles as “modus operandi,” which means a mode of being and reminds folks that it takes effort and practice to learn how to do this.
The CALM is an acronym that stands for the attitude of the MO. The “C” stands for curiosity and refers to a questioning, open attitude that asks:
What am I feeling?
How am I reacting?
Why am I thinking the way I am?
What are the goals of the people around me?
The “A” stands for acceptance and the capacity to tolerate difficult emotions and situations, without having to run away or decompensate. This is a skill that takes practice (see this book on fostering an acceptance mindset.
The “L” stands for loving compassion, which refers to adopting a general attitude of care and respect for both one’s self and others. (This book offers a wonderful resource on cultivating an attitude of mindful compassion.)
Finally, the “M” stands for motivated toward valued states of being.
This means adopting a reflective attitude: What are my goals in the short term and long term? How can I act in a way that moves me toward them? It uses the metaphor of a CALM MO flashlight to help folks internalize the idea that when they are feeling conflict and distress, they turn on the inner light and adopt a curious, accepting, loving attitude that is motivated toward adaptive outcomes.
It must be noted that this process of developing a CALM MO frame of mind that can be activated reliably and when under duress is not easy. It involves learning the skills of psychological mindfulness and developing each capacity identified. And it involves practice, first in role plays and imagination and then in real life, but not super difficult situations.
Finally, one grows into the capacity to enter the space under even difficult emotional circumstances.
Related: 13 Practical Strategies To Handle Being Mad or Angry
The Conclusion To The Series
The tour started with finding one’s self in the cave of a depressive shutdown, which is a brutal place to be. (Refer step 1) We have acknowledged the nature of depression as a state of shutdown and charted a possible path via awareness and acceptance. We focused first on getting a clear understanding of depression, neuroticism, and well-being.
Then we shifted into active, practical domains and focused on skills fostering behavioral activation, healthy lifestyles, healthy biology, more adaptive processing of emotions, reviewed the keys to fulfilling relationships, adaptive thinking and finally conclude today with deeper work on the self and developing a life philosophy that fosters both awareness of the darkness and an authentic growth-to-goodness outlook for the soul (i.e., the form of one’s life).
I hope you have found this series helpful. As everyone who has been depressed knows, it sucks, and I extend you compassion for your suffering. The magnitude of depression as a public health problem is enormous, and we all need to come together and share in offering the best we can to help reverse the cycles that feed the beast. Please share this series with anyone who might benefit. I will put a final “full summary” blog together so it can be sent with one link.
If you are in therapy and find this blog series to be of interest, please share with your therapist and discuss it so you are both on the same page. In addition, if you know someone who is depressed, perhaps this blog can be a source of education and conversation about what depression is, why people get depressed, and what they might be able to do about it. Learning how to talk about depression is an important component in learning how to deal with and prevent depression.
In addition, any discussion of depression must include awareness of the fact that significant numbers of people who are depressed have suicidal ideation. Please get help if you are dealing with suicidal thoughts or impulses (here is one resource).
If you have any questions or comments or recommendations, feel free to post them here or email me at [email protected]. I wish you all the best in your journey.
Written by:Gregg Henriques, Ph.D. What to Do If You Are Depressed. The whole series is found here on Unified Theory of Knowledge Homepage: Originally appeared on: Psychology Today Republished with permission Here are links for your reference: What to Do If You Are Depressed What to Do If You Are Depressed: Facing the Beast What to Do If You Are Depressed: Be Aware of the Paradoxes What to Do If You Are Depressed: Know Your Level What to Do If You Are Depressed: Know the Three Kinds What to Do If You Are Depressed: Identify Neurotic Loops What to Do If You Are Depressed: Assess Your Well-Being What to Do if You Are Depressed: Values Clarification What to Do If You Are Depressed: Behavioral Activation What to Do if You Are Depressed: Healthy Lifestyles What to Do If You Are Depressed: Taking Care of Your Biology What to Do If You Are Depressed: Relating to Your Emotions What to Do If You Are Depressed: Relationships What to Do If You Are Depressed: Adaptive Thinking What to Do if You Are Depressed: Identity and Shadow Work
Frequently Asked Questions
If I have depression do I need love or friends to help me?
Our loved ones can surely help us to feel better but depression is a mental health disorder that needs medical attention and/or therapy from a professional expert.
I’m dealing with depression from past trauma. What can I do to release this?
You will be well advised to seek help from a mental health professional who has experience in the area of trauma healing.
Is it good or bad if u keep yourself locked in your own room cause of depression?
It’s not advisable to keep yourself locked up in a room for a long time and especially so if you’re depressed. You need to make an effort to connect with others and seek help.
How can I make myself less insecure and not be depressed?
If you believe you’re struggling with self-image issues and depression, the best thing to do would be to consult a legitimate mental health expert.
How to get rid of anxiety or depression as a 9-year-old?
A 9-year-old will not be capable to process their emotions on their own. Counseling by a mental health professional and parental guidance would be needed.










Leave a Comment